
The most famous two minutes in sports is usually told as a story about speed, bloodlines, and tradition. Underneath all of that, the Kentucky Derby is also something else. It’s a respiratory event, one of the most extreme in mammalian biology. Once you see it that way, the race starts to tell a much more interesting story about lungs. Including yours.
What’s actually happening in those two minutes
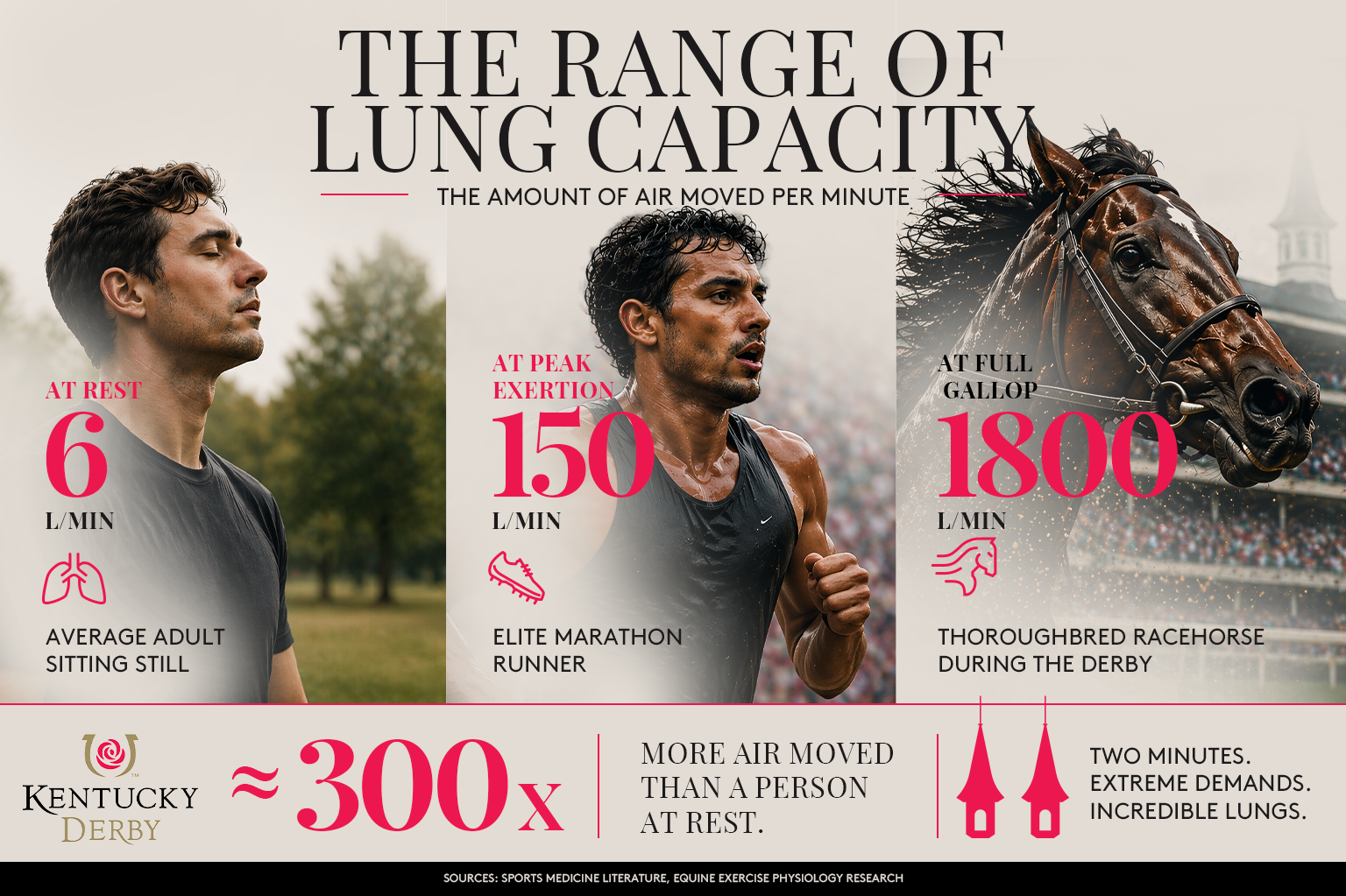
A Thoroughbred at a full gallop moves roughly 1,800 liters of air per minute through its lungs. That’s about 475 gallons. A standard bathtub holds around 40 gallons. So a racehorse at full effort is moving the equivalent of eleven bathtubs of air, in and out, every sixty seconds.
For comparison, a person sitting still breathes about six liters per minute. An elite marathon runner at peak exertion tops out around 150. The horse is doing roughly 300 times the work of the person watching it.
There’s another layer that’s even stranger. When a Thoroughbred is galloping, its breathing is locked to its stride. One breath per stride. Always. The horse cannot choose to breathe faster than it runs. The mechanics of the gallop, specifically the way the abdominal organs swing back and forth against the diaphragm, turn breathing into something the legs control rather than the lungs. At roughly 130 strides per minute during the Derby, that’s 130 breaths, each one pulling in about 12 to 14 liters of air. A resting human breath, by contrast, is about half a liter.
Multiply it out and the Derby is roughly 260 strides, 260 massive breaths, and around 3,400 liters of air moved, all within two minutes.
The lungs are not built for this without a cost. Exercise-induced pulmonary hemorrhage, or EIPH, is a well-documented phenomenon in veterinary medicine. Under the extreme demands of a race, the tiny blood vessels in a horse’s lungs can rupture, and most racehorses show some degree of airway bleeding after hard exercise. It’s one of the most studied conditions in equine sports medicine, and a reminder that even lungs built for this kind of effort reach a limit.
What the Derby can teach us about how we think about lungs
In pulmonary medicine, we measure lung function with something called a PFT, or pulmonary function test. It’s straightforward. You breathe into a mouthpiece, and a small machine measures how much air you can move, how fast you can move it, and how well your lungs are transferring oxygen into your blood. It takes about 15 to 30 minutes. It’s painless. It’s also one of the most useful tools clinicians have for evaluating breathing symptoms and supporting a diagnosis of conditions like asthma and COPD.
Now look back at the Derby. What the race reveals, at maximum effort, is the same kind of thing a PFT helps evaluate in a clinical setting: airflow, lung capacity, gas exchange, and how the heart and lungs work together under stress. The Derby isn’t a medical test, but it offers a dramatic analogy for how hard lungs can work, and how much is happening inside them that we rarely stop to think about.
There’s a larger point sitting behind all of this.
Tens of millions of American adults live with asthma. Many more have early or undiagnosed COPD. Most Americans have never had their lung function formally measured, not because they don’t need to, but because lungs are famously quiet until they aren’t. People don’t think about breathing until something feels wrong.
We study every breath of a three-year-old horse running for two minutes on the first Saturday in May. We pay almost no attention to the millions of much longer, much quieter breaths happening in the stands, in living rooms, and at watch parties all over the country.
That gap isn’t a criticism of anyone. It’s just how the system tends to work. The Derby, once you notice the asymmetry, becomes a useful mirror.
The Lasix conversation is really a conversation about cause versus symptom
For decades, the standard approach to racehorse bleeding was a medication called Lasix, known generically as furosemide, a diuretic. Administered hours before a race, it reduces the volume of blood circulating through the lungs and lowers pressure in the pulmonary capillaries. Less pressure, less bleeding. At peak, the vast majority of North American Thoroughbreds raced on it.
What Lasix doesn’t do is address what’s happening underneath. It manages the symptom in the moment and leaves the structural issue untouched.
In 2022, the Horseracing Integrity and Safety Authority banned race-day Lasix in stakes races, including the Kentucky Derby. The reasoning was that the sport should focus more on the underlying causes of EIPH, through breeding, training, and environmental changes, rather than relying on a medication to manage the effect.
It’s worth pausing here, because a version of the same conversation has been happening in human respiratory medicine for a long time.
Most people with asthma know the feeling of reaching for a rescue inhaler. It works quickly, relieves symptoms in the moment, and is one of the most widely used medications in the world. Rescue inhalers aren’t designed to treat the inflammation that drives asthma over time. Controller medications, the ones used daily whether symptoms are present or not, are the ones that address that underlying process. For patients with more complex or severe disease, newer therapies work further upstream still, targeting the biology that sets the condition in motion.
None of this means one type of medication is right or wrong. It means respiratory care, like a lot of medicine, is always balancing two questions: how do we help someone feel better right now, and how do we address what’s actually causing the problem. The Derby’s Lasix decision is a public version of a conversation that already happens quietly between pulmonologists and their patients every day.
Your own Derby Day
On the first Saturday in May, Derby Day is a respiratory event for the horses, and a respiratory environment for everyone watching. That includes anyone in Gwinnett County enjoying the race from a backyard, a patio, or a porch.
May in Georgia is peak grass pollen season. Atlanta-area grass pollen counts in early May typically land in the high range, and tree pollen is often still tailing off at the same time. That stacks two allergen sources on top of each other. For many adults in our community living with asthma, and for people whose airway sensitivity hasn’t yet been identified, that combination is not abstract. It’s the kind of day lungs notice.
Add the Derby itself. When the race is running, spectators at the track or at home tend to breathe faster, hold their breath, shout, laugh. Respiratory rate rises briefly, even for people who aren’t moving a muscle. For anyone prone to asthma symptoms or shortness of breath on exertion, that brief excitement can be a reminder of how noticeable breathing symptoms become during stress, allergen exposure, or physical effort.
This isn’t a reason to worry. It’s a reason to notice.
The quiet point underneath all of this
A lot of what we know about lungs has come from studying extreme demand: athletes, high-altitude climbers, and yes, racehorses. What that research consistently shows is that lungs do an enormous amount of work quietly, and that most people are carrying around a lot more respiratory capacity, and sometimes a lot more strain, than they realize.
Symptoms like shortness of breath on the stairs, a chronic cough that won’t quite go away, wheezing during exercise, or a slow drop in stamina are worth paying attention to. They’re the kinds of things a pulmonary function test can help evaluate.
If you’ve been noticing changes in your breathing, whether it’s getting winded more easily, a cough that’s lasted longer than it should, or shortness of breath during activities that used to feel easy, it’s worth bringing up with your provider. You can learn more about pulmonary function testing at Gwinnett Pulmonary & Sleep here. The test itself takes less time than the Derby broadcast’s pre-race coverage, and the information it provides can be useful for understanding what your lungs are doing day to day.